A common cold can make you feel tired, blocked up, sore and run down. Most colds improve on their own within about 7 to 10 days, but that does not mean you need to simply wait it out. Good self-care can help your body recover, ease symptoms and may help you feel better sooner.
It is important to be realistic. There is no instant cure for the common cold. Antibiotics do not help because colds are caused by viruses, not bacteria. The goal is to support your immune system, reduce symptom strain and avoid things that can slow recovery.
Start self-care as soon as symptoms appear
The first day or two of a cold matters. This is when symptoms often build and when your body is already using energy to fight the virus.
At the first signs of a sore throat, sneezing, runny nose or tiredness, slow down. Reduce non-essential activity, go to bed earlier and avoid pushing through a busy day if you can. Early rest may not “kill” the cold, but it can help your body use energy for recovery rather than stress, overwork and exhaustion.
Practical tips:
- Cancel or postpone non-urgent tasks.
- Keep warm and comfortable.
- Avoid intense exercise while you feel unwell.
- Work from home or rest at home if possible.
- Start fluids, saline spray and throat care early.
Prioritise sleep and rest
Sleep is one of the most useful recovery tools you have. Your immune system works actively during sleep and being sleep-deprived can make it harder for your body to recover well.
Aim for extra sleep while you are unwell. If you cannot sleep for long stretches because of coughing or congestion, rest quietly during the day. Even short rests can reduce the load on your body.
Try this:
- Go to bed earlier than usual.
- Take a short nap if you feel drained.
- Sleep slightly propped up if a blocked nose or cough is keeping you awake.
- Avoid screens, alcohol and heavy meals close to bedtime.
- Keep the bedroom comfortably cool, quiet and well ventilated.
Keep your fluids up
Fluids do not cure a cold, but they help your body function properly while it is fighting infection. Drinking enough can also help thin mucus, ease a dry throat and reduce the risk of dehydration if you have a fever.
Water is the best option. Warm drinks can also feel soothing, especially if your throat is sore or your nose is blocked.
Good options include:
- Water
- Warm water with lemon
- Herbal tea
- Broth or soup
- Warm water with honey for adults and children over 1 year
Avoid too much alcohol because it can affect sleep and contribute to dehydration. If you are not passing much urine, feel dizzy or cannot keep fluids down, seek medical advice.
Use saline spray, drops or rinse for a blocked nose
A blocked nose can make sleep difficult and leave you feeling worse. Saline nasal sprays, drops or rinses can help moisten the nasal passages, loosen mucus and make breathing through your nose easier.
Saline is not a medicated decongestant, so it is often a gentle option for many people. Use it according to the product instructions. For babies and young children, ask a pharmacist or doctor about suitable saline drops and safe mucus-clearing methods.
Practical tips:
- Use saline before bed to help with sleep.
- Use it before meals if congestion is affecting appetite.
- Choose drops for young children rather than strong sprays.
- Use sterile or previously boiled and cooled water if preparing a rinse, and follow hygiene instructions carefully.
Soothe your throat and cough

A sore throat and cough can interrupt sleep, and poor sleep can make recovery feel harder. Soothing the throat may help you rest better.
For adults and children over 1 year, honey may help calm a cough. You can take a teaspoon of honey on its own or stir it into warm water. Do not give honey to babies under 12 months because of the risk of infant botulism.
Other options include:
- Gargling warm salty water for a sore throat
- Sucking on ice chips or ice blocks
- Using throat lozenges if age-appropriate
- Drinking warm fluids
- Avoiding smoke, vaping and strong fumes
Do not give lozenges or hard sweets to young children because they can be a choking risk.
Use warm moisture safely
Warm moisture may help loosen mucus and soothe irritated airways. This can make you feel more comfortable while your body recovers.
You can try:
- A warm shower
- Sitting in a steamy bathroom
- A clean cool-mist humidifier
- Warm drinks to soothe the throat
Be careful with steam from bowls of hot water because burns can happen, especially in children. A steamy bathroom or shower is usually safer than leaning over boiling water. If using a humidifier, clean it regularly so it does not spread mould or germs
Use symptom-relief medicine safely
Pain, fever, headache and sinus pressure can make a cold feel much worse. Over-the-counter medicines such as paracetamol or ibuprofen may help relieve discomfort, but they do not cure the cold.
Use medicines carefully:
- Follow the dose instructions on the packet.
- Do not take more than one product containing paracetamol at the same time.
- Ask a pharmacist before using combination cold and flu products.
- Avoid aspirin in children and teenagers unless a doctor has specifically advised it.
- Check with a pharmacist or doctor before using ibuprofen if you have asthma, kidney disease, stomach ulcers, heart disease, are pregnant or take blood-thinning medicine.
Decongestant nasal sprays can help a blocked nose for a short time, but they should not be used for more than a few days unless advised. Overuse can cause rebound congestion, where the nose becomes blocked again when the medicine wears off.

Consider zinc early, but be cautious
Zinc is one of the few supplements with some evidence that it may shorten an ongoing cold if taken early. The evidence is not strong enough to call it a cure, and it may cause side effects such as nausea, stomach upset, mouth irritation or an unpleasant taste.
If you want to try zinc, speak to a pharmacist first, especially if you are pregnant, breastfeeding, have a medical condition or take regular medicines. Timing matters. It is usually discussed as something started within the first 24 hours of symptoms, not several days into the cold.
Important safety notes:
- Do not exceed the recommended dose on the product.
- Do not take zinc long-term unless advised.
- Avoid zinc nasal sprays or gels unless specifically recommended by a health professional.
- Stop taking zinc if it causes troublesome side effects.
Food sources of zinc include seafood, meat, poultry, dairy foods, eggs, legumes, nuts, seeds and wholegrains.
Eat simply and support your recovery
You do not need a perfect diet when you have a cold. The aim is to give your body enough energy, protein and nutrients without making meals difficult.
Choose easy, nourishing foods such as:
- Soup with vegetables and chicken, lentils or beans
- Eggs on toast
- Yoghurt with fruit
- Oats with banana
- Rice or noodles with vegetables and protein
- Smoothies if chewing feels difficult
- Citrus fruit, berries, kiwi fruit, capsicum and leafy greens for vitamin C
Vitamin C is important for immune function, but taking high doses after a cold starts is unlikely to make symptoms disappear quickly. It is better to focus on regular vitamin C-rich foods as part of your usual diet rather than relying on last-minute megadoses.
If your appetite is low for a day or two, focus on fluids and small meals. If you cannot eat or drink properly, or a child is not feeding well, contact a doctor.
What not to do when you have a cold
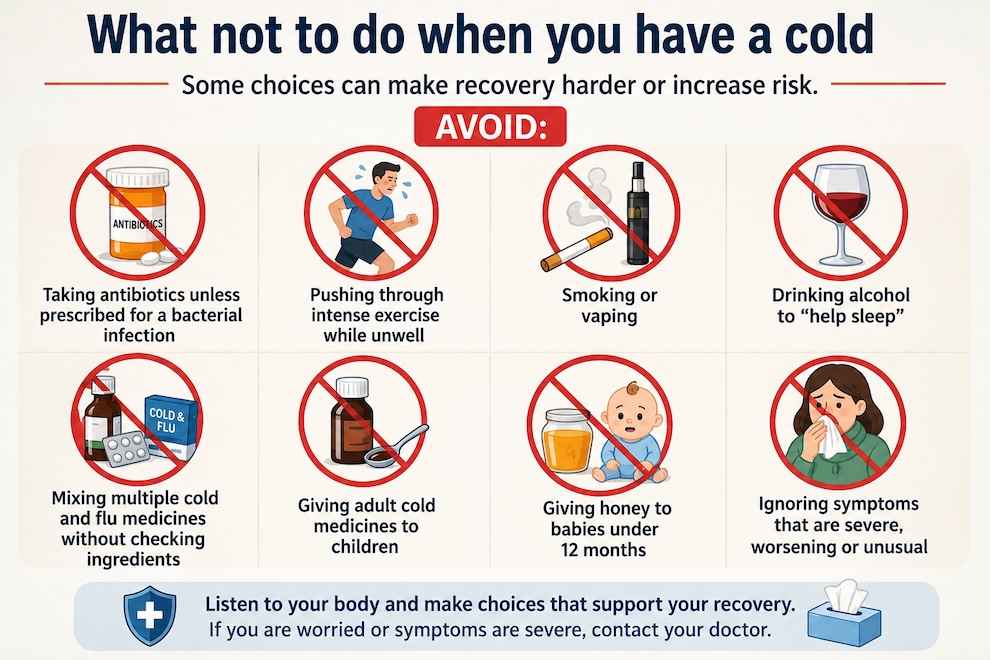
Some choices can make recovery harder or increase risk.
Avoid:
- Taking antibiotics unless prescribed for a bacterial infection
- Pushing through intense exercise while unwell
- Smoking or vaping
- Drinking alcohol to “help sleep”
- Mixing multiple cold and flu medicines without checking ingredients
- Giving adult cold medicines to children
- Giving honey to babies under 12 months
- Ignoring symptoms that are severe, worsening or unusual
When to contact your doctor
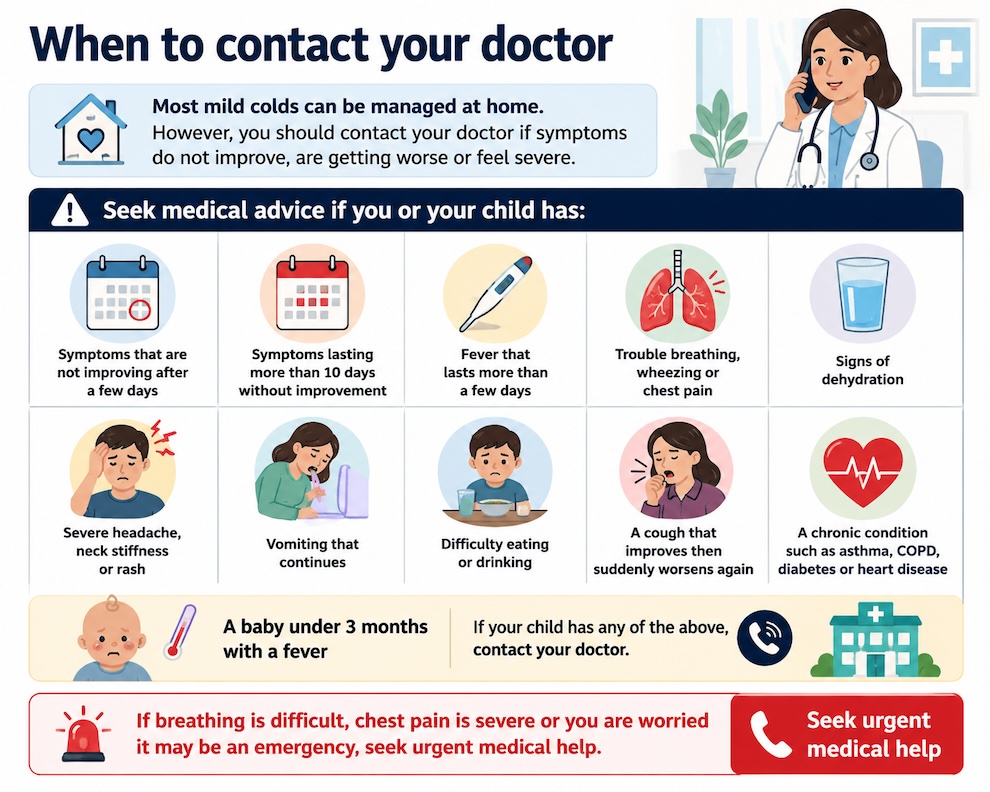
Most mild colds can be managed at home. However, you should contact your doctor if symptoms do not improve, are getting worse or feel severe.
Seek medical advice if you or your child has:
- Symptoms that are not improving after a few days
- Symptoms lasting more than 10 days without improvement
- Fever that lasts more than a few days
- Trouble breathing, wheezing or chest pain
- Signs of dehydration
- Severe headache, neck stiffness or rash
- Vomiting that continues
- Difficulty eating or drinking
- A cough that improves then suddenly worsens again
- A chronic condition such as asthma, COPD, diabetes or heart disease
- A baby under 3 months with a fever
If breathing is difficult, chest pain is severe or you are worried it may be an emergency, seek urgent medical help.
Key takeaway
You cannot force a cold to disappear overnight, but you can support your body with rest, fluids, sleep, nasal care, throat soothing and safe symptom relief. Zinc may help some people when started early, but it is not suitable for everyone. If symptoms do not improve, become severe or you are worried, always contact your doctor.
References
Abuelgasim H, Albury C, Lee JJ. (2021). Effectiveness of honey for symptomatic relief in upper respiratory tract infections: a systematic review and meta-analysis. BMJ Evidence-Based Medicine, 26(2), 57-64. doi: 10.1136/bmjebm-2020-111336
Centers for Disease Control and Prevention. (2026). Manage common cold. CDC.
Healthdirect Australia. (2024). Colds. Healthdirect Australia.
Healthdirect Australia. (2025). Medicines for colds, flu (influenza) and COVID-19. Healthdirect Australia.
Hemilä H, Chalker E. (2013). Vitamin C for preventing and treating the common cold. Cochrane Database of Systematic Reviews, 2013(1), CD000980. doi: 10.1002/14651858.CD000980.pub4
Nault D, Machingo TA, Shipper AG, Antiporta DA, Hamel C, Nourouzpour S, Konstantinidis M, Phillips E, Lipski EA, Wieland LS. (2024). Zinc for prevention and treatment of the common cold. Cochrane Database of Systematic Reviews, 2024(5), CD014914. doi: 10.1002/14651858.CD014914.pub2
Oduwole O, Udoh EE, Oyo-Ita A, Meremikwu MM. (2018). Honey for acute cough in children. Cochrane Database of Systematic Reviews, 2018(4), CD007094. doi: 10.1002/14651858.CD007094.pub5
Last reviewed and updated: 18 June 2026